Last month I talked about my disease, Crohn’s Disease. This month I will attempt to tackle the other most common disease with IBD, Ulcerative Colitis. Of course, I don’t have it so it will be hard to put my own feelings into this so it might read more like a medical journal. I apologize for that but I want you, the reader, to understand that IBD isn’t just one disease and we all go through life with IBD differently.
What is Ulcerative Colitis?
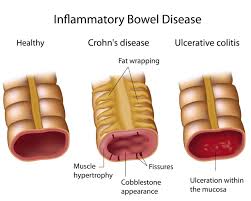
The first thing you should know is that Ulcerative Colitis or UC isn’t better or worse then Crohn’s. It is just different. Crohn’s can affect any area of the digestive track but UC only occurs in the colon. You know this by the name of the disease. Colitis actually means inflammation of the colon. Someone with CD might hear they have Crohn’s Colitis and get confused. This just means that the Crohn’s is in the colon. With UC, not only is the colon inflammed but also has ulceration. The other difference between the CD and UC is that CD can affect all layers of the bowel wall but UC will just affect the lining of the intestines.
Diagnosing
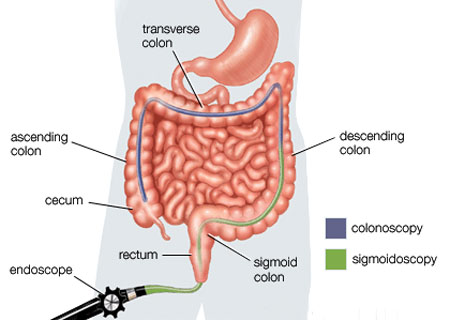
The first step in diagnosing UC is usually doing blood and fecal matter tests. They will test your stool for reasons for diarrhea and blood like bacteria, viruses and parasites. The next step would be endoscopy. This might consist of a sigmoidoscopy or a total colonoscopy. During the scope, like with CD, the doctor will probably take a biopsy.
Symptoms
While both UC And CD are IBD, they don’t have all the same symptoms. Crohn’s seems to have a lot more since it affects more of the body. There are many that they do share though.
- Bowel movement become looser and more frequent – Diarrhea is common and like CD is hard to control.
- Blood stool – Because of the ulceration and inflammation, there will be blood in the stool.
- Abdominal pain – Because this is a gut disease, there will be pain in the abdomen. At times it can be crippling.
- Lack of appetite – Of course, because of what is going on in the colon, you might not have much of an appetite. Many people actually feel pain when they eat also and tend not to eat to avoid the pain.
- Weight loss – Between not eating and diarrhea, wight loss is expected and does happen. With many people it can be a drastic weight loss.
- Fatigue – Because your body is fighting itself, you will feel tired. There are times when a person with UC will have no energy. This is normal.
Cause of Ulcerative Colitis
The big question of the day….what causes UC? The answer to this is….no one knows. Sadly, it is not know what causes UC or any IBD for that matter. Some say it is the environment, while others will say genetics and still others will say it is the food we eat. To date, there have been no hard evidence showing what causes Ulcerative Colitis. There have been studies done on this however. Once study was done by CCFA:
Research sponsored by CCFA has led many scientists to believe that ulcerative colitis may be the result of an interaction of a virus or bacterial infection of the colon and your body’s natural immune system response. Normally, your immune system will cause temporary inflammation to combat an illness or infection, and then the inflammation will be reduced as you regain health. In people with ulcerative colitis, however, this inflammation can persist long after your immune system should have finished its job.
Like CD, UC affects many people. In the USA alone there are around 700,000 people affected by UC. It is equally distributed between men and women so sex is not a factor. Unlike CD that usually shows up early in life usually in your teenage years, UC is usually diagnosed when the person is in their mid 30’s. That isn’t to say you can’t get it at an earlier age as there are many kids with UC.
Medicines
Again, to make it easy, I will quote from the CCFA’s website on the types of medicines used:
Aminosalicylates (5-ASA)
These include medications that contain 5-aminosalicylate acid (5-ASA). Examples are sulfasalazine, mesalamine, olsalazine, and balsalazide. These drugs are not specially approved by the Food and Drug Administration (FDA) for use in ulcerative colitis.. However, they can work at the level of the lining of the GI tract to decrease inflammation. They are thought to be effective in treating mild-to-moderate episodes of ulcerative colitis and useful as a maintenance treatment in preventing relapses of the disease. They work best in the colon and are not particularly effective if the disease is limited to the small intestine.
Corticosteroids
Prednisone, methylprednisolone and budesonide are steroids that are available orally and rectally. Prednisone and methylprednisolone nonspecifically suppress the immune system and are used to treat moderate to severely active ulcerative colitis. (By “nonspecifically,” we mean that these drugs do not target specific parts of the immune system that play a role in inflammation, but rather, that they suppress the entire immune response.) These drugs have significant short- and long-term side effects and should not be used as a maintenance medication. Budesonide is a steroid that is used to treat localized inflammation. It has the benefit of minimal systemic exposure with far fewer risks and side effects. Because corticosteroids cause the adrenal glands to slow or stop the natural production of the human steroid cortisol, they cannot be stopped abruptly. If you cannot come off steroids without suffering a relapse of your symptoms, your doctor may need to add some other medications to help manage your disease.
Immunomodulators
This class of medications modulates or suppresses the body’s immune system response so it cannot cause ongoing inflammation. Immunomodulators generally are used in people for whom aminosalicylates and corticosteroids haven’t been effective or have been only partially effective. They may be useful in reducing or eliminating the need for corticosteroids. They also may be effective in maintaining remission in people who haven’t responded to other medications given for this purpose. Immunomodulators may take several months to begin working.
Antibiotics
Antibiotics may be used when infections—such as abscesses—occur. They can also be helpful with fistulas around the anal canal and vagina. Antibiotics used to treat bacterial infection in the GI tract include metronidazole, ampicillin, ciprofloxacin, others.
Biologic Therapies
These therapies represent the latest treatment class used for people suffering from moderate-to-severe ulcerative colitis. These treatments are called biologics because, unlike chemical medications, they are made out of material found in life, usually proteins. Many biologic treatments are proteins called antibodies, which normally are part of the body’s immune defense. The antibodies used for biologic therapy have been developed to bind and interfere with the inflammatory process in the disease.
Another thing, like CD, that can help is a change in diet. Again, food does not cause or heal UC but can help in the body to heal itself. Some foods might make it hard on the intestines like high fiber so a low fiber diet might help some people.
Surgery
In UC patients, there might come a time when meds and diet doesn’t help anymore. When this happens surgery is usually the next option. Sadly there is no simple surgery and the results are the removal of part or all of the colon and possibly the rectum. I will get into this more in another post.
One thing I do want to say about surgery, and I know many people will disagree with me on this, but even if you remove the disease from the colon, you are not cured. Like CD, UC doesn’t travel so if you remove the disease intestines, yes, the actual disease is no longer there. Because the disease is more then just in the intestines, you still carry the disease within your blood and DNA. Also, some would say removing the colon and wearing an ostomy isn’t a real cure either because you are exchanging one problem with another.
Types of Ulcerative Colitis
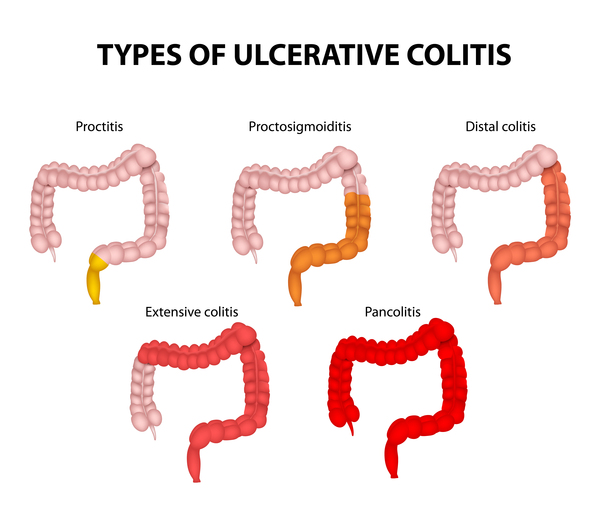
Like Crohn’s, there is no one type of UC. Instead there are a number of different types, depending on the location of the disease. According to medicinenet.com the different types are:
-
Ulcerative proctitis refers to inflammation that is limited to the rectum. In many patients with ulcerative proctitis, mild intermittent rectal bleeding may be the only symptom. Other patients with more severe rectal inflammation may, in addition, experience rectal pain, urgency (sudden feeling of having to defecate and a need to rush to the bathroom for fear of soiling), and tenesmus (ineffective, painful urge to move one’s bowels caused by the inflammation).
-
Proctosigmoiditis involves inflammation of the rectum and the sigmoid colon (a short segment of the colon contiguous to the rectum). Symptoms of proctosigmoiditis, like that of proctitis, include rectal bleeding, urgency, and tenesmus. Some patients with proctosigmoiditis also develop bloody diarrhea and cramps.
-
Left-sided colitis involves inflammation that starts at the rectum and extends up the left colon (sigmoid colon and descending colon). Symptoms of left-sided colitis include bloody diarrhea, abdominal cramps, weight loss, and left-sided abdominal pain.
-
Pancolitis or universal colitis refers to inflammation affecting the entire colon (right colon, left colon, transverse colon and the rectum). Symptoms of pancolitis include bloody diarrhea, abdominal pain and cramps, weight loss, fatigue, fever, and night sweats. Some patients with pancolitis have low-grade inflammation and mild symptoms that respond readily to medications. Generally, however, patients with pancolitis suffer more severe disease and are more difficult to treat than those with more limited forms of ulcerative colitis.
-
Fulminant colitis is a rare but severe form of pancolitis. Patients with fulminant colitis are extremely ill withdehydration, severe abdominal pain, protracted diarrhea with bleeding, and even shock. They are at risk of developing toxic megacolon (marked dilatation of the colon due to severe inflammation) and colonic rupture (perforation). Patients with fulminant colitis and toxic megacolon are treated in the hospital with potent intravenous medications. Unless they respond to treatment promptly, surgical removal of the diseased colon is necessary to prevent colonic rupture.
Like Crohn’s, getting a diagnosis of Ulcerative Colitis does not mean your life is over. With treatment you can go on to live a long and prosperous life. I know many people with UC that go on to run marathons, climb mountains and participate in iron men competitions.