So the first thing I want to say about this, is that everything I am going to write is from information gotten online. I don’t have an ostomy so I don’t have first hand experience with them. Forgive me if my information is incorrect or out of date. In fact, please let me know if something is wrong.
Let’s jump right in. What is an ostomy? According to the United Ostomy Association of America, Inc, or UOAA, an ostomy refers to the surgically created opening in the body for the discharge of body wastes. A stoma is the actual end of the ureter or small or large bowel that can be seen protruding through the abdominal wall.
There are many types of ostomies. The most common are Colostomy, Ileostomy, and Urostomy.
Colostomy: The surgically created opening of the colon (large intestine) which results in a stoma. A colostomy is created when a portion of the colon or the rectum is removed and the remaining colon is brought to the abdominal wall. It may further be defined by the portion of the colon involved and/or its permanence.
Ileostomy: A surgically created opening in the small intestine, usually at the end of the ileum. The intestine is brought through the abdominal wall to form a stoma. Ileostomies may be temporary or permanent, and may involve removal of all or part of the entire colon.
Urostomy: This is a general term for a surgical procedure which diverts urine away from a diseased or defective bladder. The ileal or cecal conduit procedures are the most common urostomies. Either a section at the end of the small bowel (ileum) or at the beginning of the large intestine (cecum) is surgically removed and relocated as a passageway (conduit) for urine to pass from the kidneys to the outside of the body through a stoma. It may include removal of the diseased bladder.
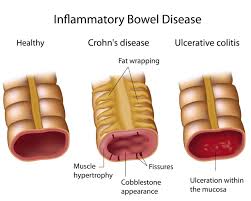
Now, the first two types, Colostomy and Ileostomy, are the 2 types most common with IBD. Urostomy is more with urinary track issues.
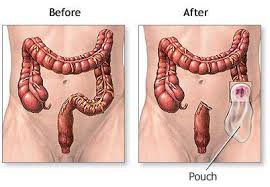
You might be thinking, ok, now that a stoma is sticking out of the body where does the product coming out go. Well, the intestine that the stoma is part of is still active and product will come out so it has to be caught in a pouch. According to the UOAA there are different types.
Colostomy and Ileostomy Pouches: Can be either open-ended, requiring a closing device (traditionally a clamp or tail clip); or closed and sealed at the bottom. Open-ended pouches are called drainable and are left attached to the body while emptying. Closed end pouches are most commonly used by colostomates who can irrigate (see below) or by patients who have regular elimination patterns. Closed end pouches are usually discarded after one use.
Two-Piece Systems: Allow changing pouches while leaving the barrier/wafer attached to the skin. The wafer/barrier is part of a “flange” unit. The pouches include a closing ring that attaches mechanically to a mating piece on the flange. A common connection mechanism consists of a pressure fit snap ring, similar to that used in Tupperware™.
One Piece System: consist of a skin barrier/wafer and pouch joined together as a single unit. Provide greater simplicity than two-piece systems but require changing the entire unit, including skin barrier, when the pouch is changed.
With an ostomy comes many psychological issues. IBD is never easy on the body or mind and an ostomy just adds to the issues. The following are some issues according to the OUAA.
A. Patient’s Concerns about Surgery
The reaction to intestinal or urinary diversion surgery varies from one individual to the other. To some, it will be a problem, to other, a challenge; where one person considers its life-saving, another finds it a devastating experience. Each person will adapt or adjust in their own way and in their own time.
Body Image/Self-Esteem Concerns
Permanent and significant changes in the body’s appearance and functional ability may change the way the person internalizes their body image and self-concept.
Fear of loss is normal and facing any loss is difficult. What are patients giving up by having this operation? Is there any gain? How changed will they be? Such thoughts may lead to weeping or depression, or they may be denied.
It is important to understand the impact of the ostomy surgery on the patient’s change in self-image and how they perceive themselves. It may be accepted as the lesser of two evils, or they may refuse to acknowledge its existence, or may hold onto the belief that it is a temporary situation.
Within the rehabilitation process there are times that patients should have the opportunity to express or deny their feelings, about their surgery, the changes in their body or their self-image.
Self-Care Concerns
Patients have to be reassured that they will be taught self-care and that they will be able to master the management process. Basic anatomy and physiology should be explained to new patients, so they can better understand the extent of their surgery. Management options should be offered.
Patients should begin to assist the ostomy nurse with caring for the ostomy as soon as possible. Becoming involved in this process will begin to build confidence and help the patient to regain control of his situation.
Relationship Concerns
Patients may fear that their social role may be changed and that others may not accept them as in the past. One of the first concerns seems to be how to tell others about your surgery, who to tell and when.
• Patients should be prepared to explain their surgery with a few brief statements such as, “An ostomy is a surgical procedure for the diversion of bowel (or bladder).”
• They should understand that they do not have to tell everyone about the surgery. Be selective about who and how much to tell. It may be only to friends who will be supportive throughout the rehabilitation process.
Returning to the work place may present a concern about restroom facilities, interaction with co-workers, and feelings of being “watched.”
• Maybe a few of their co-workers may need to know in the event of an emergency.
• Employability and insurability are issues for some individuals. If these issues develop, seek help from healthcare professionals and/or talk with others who have found solutions to any of these issues.
Sexuality issues are common concerns for the new ostomate. Linked closely to our feelings of sexuality is how we think about ourselves and our body image.
• Any sexuality concerns should be discussed between the patient and his partner. It is likely that the partner will have anxieties due to a lack of information. An intimate relationship is one in which it matters how well two people can communicate about the most personal of human functions, that is, bodily elimination and sex.
• Ostomy surgery may present more concerns for single individuals. When to tell depends upon the relationships. Brief casual dates may not need to know. If the relationship grows and leads to intimacy, the partner needs to be told about the ostomy prior to a sexual experience.
B. Phases of Psychological Adaptation
Almost every patient goes through four phases of recovery following an accident or illness that results in loss of function of an important part of the body. The patient, along with the family, goes through these phases, varying only in the time required for each phase. People may experience the various phases of adaptation in a different order and at varying rates. Some people may skip certain phases entirely and some may move up and down at different times.
These phases are shock, denial, acknowledgment and resolution.
1. Shock or Panic
Usually occurs immediately after surgery. The patient is unable to process information and may be tearful, anxious and forgetful. This phase may last from days to weeks.
2. Defense/Retreat/Denial
This phase may last for weeks or months and delays the adaptation process. During this phase, the individual denies or minimizes the significance of the event and defends himself against the implications of the crisis. You may note the avoiding of reality and “wishful” thinking.
3. Acknowledgment
As the patient moves to the next step of acknowledgment, he begins to face the reality of the situation. As you give up the existing old structure, you may enter into a period, at least temporarily, of depression, of apathy, of agitation, of bitterness, and of high anxiety.
4. Adaptation/Resolution
During this phase, the acute grief begins to subside. The patient copes with their situation in a constructive manner and begins to establish new structures. They develop a new sense of worth. This phase may take one to two years.
With the aid of an ostomy nurse and the ostomy visitor, you learn about living with a stoma.
One thing I can say about ostomies, they are not the end of the world and not the end of your life. In fact, and I have heard this from many people, is that once you get one it usually gives you back your life. People with IBD get ostomies because they are in dire straits and can’t live their life. They are having many problems with their disease and usually in constant pain. By getting the ostomy, the disease part of their intestines is removed and a lot of their problems are gone. That isn’t to say all of their problems are gone and with ostomies, a whole new set of problems can occur, with dehydration the biggest one. But overall, most people can begin to live a pain free life and can once again do things they couldn’t before.
As I mentioned I used the UOAA site for this information. Their site can be found here http://www.ostomy.org/Home.html.